 Ultrasound scanner technology continued to develop and improve in the 1980s. Realtime scanners had rather standard appearance, sizes and fabrication. They are usually portable on 4 wheels with the monitor on the top of the console and rows of receptacles at the bottom to accomodate a variety of scanner probes.
Ultrasound scanner technology continued to develop and improve in the 1980s. Realtime scanners had rather standard appearance, sizes and fabrication. They are usually portable on 4 wheels with the monitor on the top of the console and rows of receptacles at the bottom to accomodate a variety of scanner probes.
Prior to the 1990s, B-scan ultrasound images made steady progress in resolution and quality, but the improvements were not dramatic and except for a few really top-end brands, images in the late 1980s did not have significant improvements over those in the early 80s. During this period, techiques for resolution and overall image enhancement centered around the increase in the number of transducer crystals (or channels, from 64 to a maximum of 128), improvements in transducer crystal technology (going into broad-band and high dynamic range), increasing array aperture (more crystals firing in a single time-frame (with faster computational capabilities), improving technical agorithms for focusing on receive (increasing the number of focal zones along the beam), incoporating automatic time-gain controls and progressively replacing analog portions of the signal path to digital.
Image quality saw some real improvements in the early to mid 1990s. The availability of new and effective technologies to ultrasound scanners had progressively stemmed from advances in technology in other areas of science such as radar navigation, telecommunications and consumer electronics. Such included the rapid developments in cellular telephones, micro-computers, digital compact and versatile disk players, and high definition TVs. The very high-speed digital electronics required for ultrasound application had become available at an affordable costs. The ultrasound imaging market alone would not have supported the development of these new technologies.
The new developments include:
1. The entire signal processing chain becomes digital. The entire signal chain which includes:
[ the transducer ] --> [ beamformer ] --> [ signal processor ] --> [ scan converter ] --> [ Monitor ] all operate in digital electronics.
 Previously the beamformer (employing analog delay lines) and the signal processing stages are usually analog in their operation. The digital change-over was based on the very powerful computer platforms that were only available after the mid 1990s. The processor in the newer highend machines has the power equivalent of roughly 40 Pentium processors, executing some 20 to 30 billion operations per second. Most of the processing are also programmable software-based rather than hardware-based and allow for much more versatility and finer adjustments in the manipulation of beam signals. Signals from and to the transducer elements are digitized before any signal processing, which is one of the most important advancement in ultrasound technology in the 90s. It opened the venue for dealing with some of more difficult areas in ultrasound physics.
Previously the beamformer (employing analog delay lines) and the signal processing stages are usually analog in their operation. The digital change-over was based on the very powerful computer platforms that were only available after the mid 1990s. The processor in the newer highend machines has the power equivalent of roughly 40 Pentium processors, executing some 20 to 30 billion operations per second. Most of the processing are also programmable software-based rather than hardware-based and allow for much more versatility and finer adjustments in the manipulation of beam signals. Signals from and to the transducer elements are digitized before any signal processing, which is one of the most important advancement in ultrasound technology in the 90s. It opened the venue for dealing with some of more difficult areas in ultrasound physics.
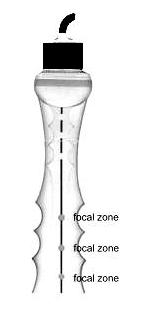
Superfast digital beamformers allow for many times the number of focal points along the beam and produce microfine focal points on receive to the size of a screen pixel. Digital beamforming also reduces noise in the signal processing by several hundred folds producing a much cleaner picture.
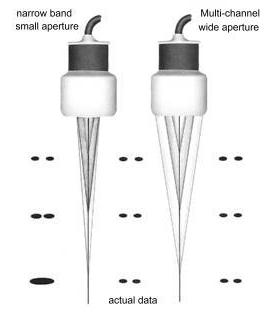
2. Extensive use of refined broad-band wide aperture transducers, improving both definition of tissue textures and dynamic range. With wide aperture transducers, transmit and receive apodization also allowed for the electronic reduction of the lateral array elements (sidelobes). In the early 1990s there was much improvements in transducer material design and fabrication technology allowing for higher frequency transducers, improved sensitivity and contrast resolution. The number of channels in high-end systems went up to 256 and more recently to 512 and 1024 (2-D arrays) in several high-end systems allowing for extremely wide aperture on transmission and reception. In ultrasound physics, the lateral resolution is the product of the wavelength and the f-number. The f-number equals the depth of the returning echo divided by the aperture of the beam. (the aperture of the beam is the width of the number of simultaneous firing transducer elements in the array, that means the larger the aperture the more elements are fired simultaneously). Therefore lateral resolution will be best (smallest) if there is a large aperture and short wavelength (higher frequency). Too large an aperture will slow the frame rate considerable and requires very fast computation and parallel processing. This has been made possible with the more recent digital electronics and the very powerful super-processors (see above). Many slightly older ultrasound systems are capable of using low f-numbers on reception at an affordable cost. However, they often employed large f-numbers on transmit in order to cover a large area. Significant improvement in lateral resolution requires low f-numbers both on transmit and receive. With the new 'very wide' aperture beamformer (often up to 128 channels), the transmit and receive f-numbers are both lowered. The resulting improvements in lateral resolution can be as much as 4 times.
3. The phase data in returning ultrasound echoes, in addition to the amplitude data are processed in what is known as coherent imaging. The technique produced twice the amount of data from which to create ultrasound images of high resolution. The late 1990s has also seen transducer developing into 2D arrays which is made up of large number of elements arranged in rows and columns across the face of the transducer. Focusing occurs in two directions which produced a finer and clearer definition in both planes eliminating artifacts from adjacent tissue planes which may be slightly different.
4. The advent of tissue harmonic imaging. The technology, which has emerged as a major imaging trend in the last 2 years of the 1990s, made used of the generation of harmonic frequencies as an ultrasound wave propagates through tissue, dramatically reducing near field and side lobe artifacts. As ultrasound waves propagate through tissue, there is non-linearities in sound propagation that gradually change the shape of the wave, a shape change that can only result from the development of harmonic frequencies within the wave. There are no harmonic frequencies present at the transducer face. They develop gradually as the wave propagates through tissue, and so in the near field there is very little harmonic energy available for reflection from tissue. Since the near field is a source of much of the artifact in the ultrasound image, selective display of harmonic energy will show dramatically less near-field artifact. The strength of the harmonic energy generated is proportional to the square of the energy in the fundamental wave. Most of the harmonic energy results from the strongest part of the beam, and weaker portions of the beam (side lobes, for example) generate relatively little harmonic energy. selective harmonic imaging will yield a dramatically cleaner contrast between adjacent tissue structures. The development of harmonic imaging would not have been possible until the late 1990s as there must be excellent beam linearity on transmission and super sensitivity and dynamic range on receive to display the harmonic energy without an unacceptable amount of noise, as the harmonic signals are always much less in amplitude than the original fundamental signal. There must also be a very selective and fast digital filter within the receiver, to exclude the large percentage of the fundamental signal. Harmonic imaging is particularly used in obese patients.Further refinements in harmonic imaging techniques and cost-cutting would be expected in the next few years.
Back to History of Ultrasound in Obstetrics and Gynecology.